Preparation: Plan to spend 45 minutes to an hour familiarizing yourself with the background information below, key findings on the ultrasound clips and the progressions of animations on the PowerPoint. This conference is intended as an introduction to clinical application of cardiac US and the second in our POCUS case conference series.
How to present: Present the PowerPoint by downloading the PowerPoint file (the US clips do not function in PowerPoint browser windows). Have the image pulled up in presenter mode before learners look at the screen to avoid revealing the diagnosis. Each case progresses through three or more questions, beginning with an overall interpretation, identification of a generalizable rule, and a clinical integration question. We recommend a pair-share structure with a junior and senior trainee. For each successive question, the presenter can elect to have pairs discuss their thoughts then ask for a volunteer to share or, to expedite the conference, simply ask for an audience response. Ask a learner to provide an overall interpretation. Advance using the keyboard arrows or mouse click to reveal subsequent questions and then answers with their accompanying graphics. You can go back to prior graphics and questions by using the back arrow or scrolling back on the mouse wheel.
Case 1: Severely reduced LVEF using EPSS (PLAX)
POCUS image/clip interpretation:. Global hypokinesis of LV with severely reduced LVEF and enlarged left atrium.
Clinical diagnosis: Acutely decompensated heart failure with reduced ejection fraction (HFrEF)
Teaching:
- Gross assessment of LV systolic function includes assessment of wall thickening and reduction in chamber size. An enlarged left atrium (larger than the LVOT and RV, ‘rule of thirds’) suggests increased left atrial pressures and may corroborate findings of reduced LV EF. However, an enlarged LA may also be due to mitral valve disease or LV diastolic dysfunction.
- E-point septal separation (EPSS) is an additional method to more objectively evaluate LV systolic function. The minimum distance between the anterior mitral valve leaflet and the septum is measured using M-mode.
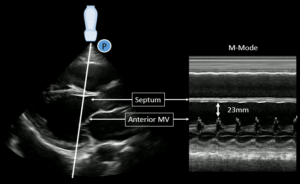
Increasingly large EPSS measurements correlate with worse systolic function:
- EPSS <7mm suggests a normal systolic function.
- EPSS >13mm suggests mod-severely reduced EF
Pitfall: EPSS may be over-estimated due to mitral stenosis, aortic regurgitation or a misaligned M-mode.
Case 2: RV strain from pulmonary embolus (PSAX)
POCUS image/clip interpretation: Parasternal short axis (PSAX) with dilated RV with flattened intraventricular septum (“D-sign) suggestive of RV strain.
Clinical diagnosis: RV strain in the setting of acute chest symptoms and shock, concerning for a massive pulmonary embolus.
Teaching:
- PSAX is the preferred view to identify RV strain with a dilated RV and flattened interventricular septum or “D-sign”.
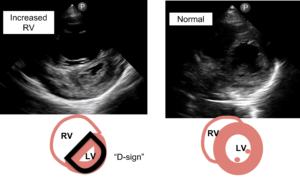
Pitfall: An off-axis PSAX may give the false appearance of a flattened septum. Always confirm the finding at multiple levels and views.
- The differential for increased RV pressure relative to the LV includes:
- Acute pulmonary embolus
- Chronic pulmonary hypertension
- RV systolic dysfunction
- Pulmonic valve disease
- The differential for increased RV pressure relative to the LV includes:
Case 3: Small pericardial effusion (PLAX)
POCUS image/clip interpretation – Parasternal long axis with small circumferential simple pericardial effusion. Normal left ventricular chamber size and function. Normal left atrial chamber size.
Clinical diagnosis – Suspected viral pericardial effusion without hemodynamic significance and no evidence of LV dysfunction to explain the patient’s presentation.
Teaching:
- In the PLAX view, a pericardial effusion is anterior to the aorta while a pleural effusion is posterior to the aorta.
- Most pericardial effusions do not cause tamponade physiology.
- The common clinical features of tamponade are JVD, tachycardia, and pulsus paradoxus >10.
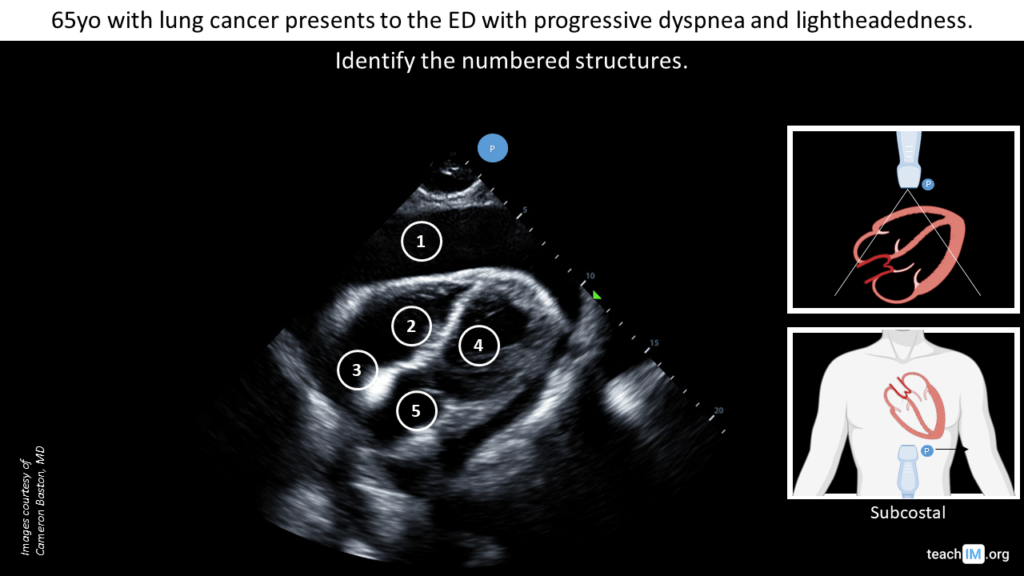
Case 4: Malignant pericardial effusion with tamponade physiology (subcostal)
POCUS image/clip interpretation:. Large circumferential pericardial effusion with diastolic collapse of the right ventricle. Normal LV systolic function.
Clinical diagnosis: Malignant pericardial effusion with clinical tamponade.
Teaching:
- Subcostal cardiac view is the most sensitive view for identifying pericardial effusion.
- Ventricular diastole occurs when the tricuspid and mitral valves are open.
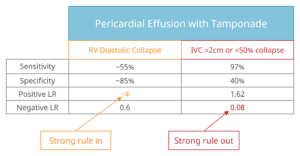
- Diastolic collapse of the RV has good rule in value (+LR 4) and the absence of a plethoric IVC (>2cm and <50% collapsing) has good rule out value (-LR 0.08) for the diagnosis of tamponade.