There are no firm recommendations to order routine screening labs. However, consider the following tests for new-onset depression or anxiety:
CBC – looking for Anemia as a cause for fatigue, low energy, poor concentration
TSH – especially if there is a family history of autoimmune or thyroid disorders.
HCG – To evaluate for a potential cause of mood disorders and inform the safest potential pharmacologic treatment.
BMP – If there is a concern for renal dysfunction and the potential need for renal dosing.
Objective 3: Construct a basic treatment strategy for Generalized Anxiety Disorder and Unipolar Depressive Disorder, including monitoring and follow-up timeline after initiation of pharmacological and non-pharmacological therapy.
Generalized Anxiety Disorder and Unipolar Major Depressive Disorder share a similar treatment algorithm for first-line therapy, each with comparable response rates to medications or psychotherapy, and the combination is additive. This algorithm is based on recommendations from the American Psychiatric Association and the Anxiety and Depression Association of America.
After identifying the patient’s target for treatment and selecting a medication and/or psychotherapy based on patient clinical features, comorbidities and preferences, it is imperative that the provider establishes clear expectations for the intervention and plans for close follow-up to assess side-effects and response to therapy.
The first couple of weeks after initiating a new pharmacologic agent (especially for first-time treatment) are critical to a patient’s safety and engagement. They may become suicidal or manic, or stop taking the medication due to undesired (but temporary) side effects or insufficient response. These negative outcomes may be prevented with a short-term follow-up with the prescribing provider, RN, or psychotherapist.
Many patients will ask about the timeline for discontinuation of these medications. While a trial of discontinuation is reasonable, recent research (N Engl J Med 2021; 385:1257) suggests that relapse and restarting antidepressants is common after discontinuation (though of note, relapse is ALSO common in patients who continue antidepressants). These meds should be tapered slowly if stopped, as withdrawal is common and can be prolonged.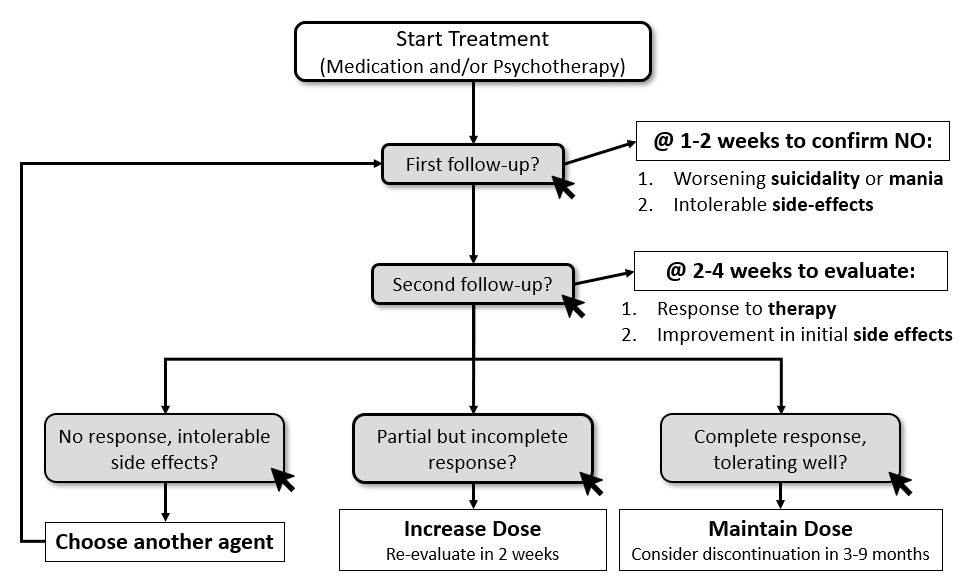
Objective 4: Select the appropriate pharmacologic therapy for anxiety or depression based on key clinical features and patient preferences.
Serotonin reuptake inhibitors, particularly SSRIs, seem to have the best safety and tolerability profile, although the evidence for this is conflicting. Key factors to consider include cost, patient preference, prior response to medication, and side effects. The interactive table helps categorize medications on their defining features (activating/sedating) and common side effects, which can often be used as an advantage. To review these options, we offer three brief vignettes to highlight common clinical situations with a selection of the most appropriate agents.
Cases
Case 1: This case highlights a typical diagnosis and treatment of a patient with new onset depressive disorder. For screening, he should be screened with a PHQ-9 due to high clinical suspicion. Take note to tell your learners that the PHQ-2 and PHQ-4 are used for generalized assessments for all patients. Given this patient’s high clinical probability, we would recommend the PHQ-9. This screening form also highlights that screening tools are inadequate for diagnosing GAD and Depression. The next question in this case gives you an opportunity to discuss Suicide Risk Assessments (see below). This case concludes with starting a patient on medication based on general recommendations (SRI as first line) and side effects (avoiding paroxetine in the setting of increased appetite.
Safety Assessment
The ability to predict attempted or completed suicide is poor, however suicide risk assessments remains a critical aspect of treating depression. Many tools exist to assess suicidal risk, make sure to discuss your site’s current process.. Importantly, encourage your learners to use straight forward language when discussing suicide, i.e. ask “are you having thoughts of killing yourself right now?”, instead of “hurting yourself?”. Also note that asking about suicide does not increase the risk or rates of suicide. We recommend having learners discuss and develop screening questions that they have used or seen used.
Take-Home Points
-
- Do not use PHQ-4 or PHQ-2 when the probability for depression or anxiety is high. Use a more in-depth tool such as GAD-7 or PHQ-9.
- Familiarize your learners with screening for suicide risk factors.
- Use side effect profile to help pick initial medication treatment