1 Assistant Professor, Department of Medicine, University of Colorado
2 Assistant Professor, Division of Pulmonary and Critical Care, Director of Ultrasound Training for the Department of Medicine, University of Pennsylvania
Objectives
- Match lower extremity vascular anatomy with the corresponding standard ultrasound views.
- Demonstrate proper image interpretation and clinical decision making for DVT POCUS using brief clinical cases.
- Demonstrate proper image acquisition of continuous (3-point) lower extremity DVT POCUS with directly-observed hands-on practice.
Teaching Instructions
Plan to spend at least 30 minutes preparing for this talk. There are three stages to this training experience.
1. Pre-work (see the section below): have the learners watch a brief introductory video and review the 1-pager handout.
2. Briefly (~15 minutes) present on proper transducer selection, patient positioning, vascular anatomy, and practice cases using the interactive PowerPoint presentation below. This should reinforce and build on the pre-work.
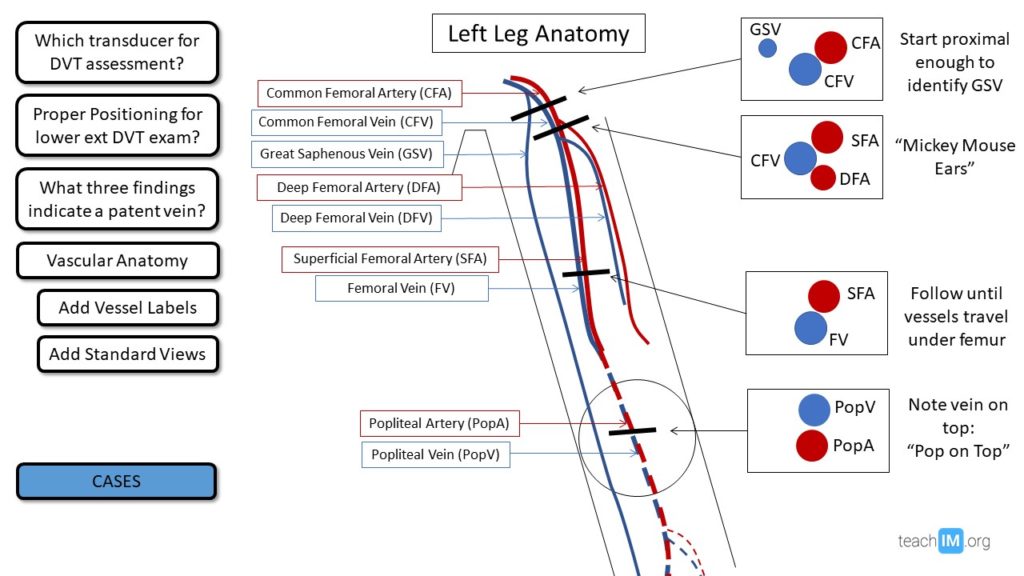
Using the buttons on the left side of the screen you can toggle graphics on and off. The most challenging part of the DVT exam is getting familiar with the anatomy. Focus on the relative relationship of an artery to a vein. With common femoral and superficial femoral, the vein is medial and/or deep to the artery. In contrast, the popliteal vein is on top of the artery (“Pop on Top”). Given the multiple branches of each vessel and anatomic variability between patients, there is plenty of opportunity for confusion around this. A reliable method to get re-oriented is to trace the vessel back up to the common femoral and slowly move down again from there.
Plan on 5 minutes for the button graphics then move onto the cases. This is an opportunity to reinforce basic image interpretation and open discussion on how to integrate these findings in clinical practice.
Case 1 demonstrates the impact of confirming the diagnosis at the bedside which introduces the option of proceeding with anticoagulation while you await a non-urgent vascular study. We still believe it is valuable to obtain a formal ultrasound as not all subsequent providers will be comfortable treating without it and a formal study will be valuable as a baseline to compare with future studies if further decision-making challenges arise later on around anticoagulation failure or consideration of discontinuation.
Case 2 presents a case of a likely pulmonary embolus based on a LE DVT identified at the bedside. This presents multiple challenges in management. We take the approach of how to empower an outpatient provider to still manage this patient as an outpatient by using the PESI score to risk stratify and have an educated risk-benefit discussion with the patient while the provider initiates anticoagulation and obtains formal studies.
3. Directly observe hands-on practice with image acquisition, either with learners practicing on each other or willing patient models. The three most common mistakes we observe and recommend focusing on are:
1. Misidentification of vein vs. artery when the vessels branch
2. Inability to elicit a doppler signal with the transducer perpendicular to the direction of blood flow
3. Not angling the transducer toward a deep bony structure to compress against.
Pre-work
The day before you plan to do in-person POCUS training ask your learners to:
- Watch this 5-minute video from Core Ultrasound.
- Review this DVT POCUS 1-pager handout
Interactive Boards
For Teaching
Use for Presenting.
DOWNLOAD FILE and USE DESKTOP APP for best performance. Otherwise, videos will not function properly.
Take Home Points
- POCUS assessment for a lower extremity DVT is a teachable exam skill with significant potential to impact clinical decision making.
- Demonstration of an anechoic and compressible vein with a doppler signal rules out a DVT at that particular site
- Compression and Doppler ultrasound at the common femoral vein, (superficial) femoral vein, and popliteal vein (3-point exam) has a > 90% sensitivity and specificity for deep vein thrombosis in beginner users with limited training.
References
Baston D. Pocket Guide to POCUS: Point-of-Care Tips for Point-of-Care Ultrasound. 1st edition. Ney York City, NY. McGraw-Hill Education; 2019
Soni NJ. Point of care ultrasound. 2nd edition. ed. St. Louis, MO: Elsevier; 2019.
Fischer EA, Kinnear B, Sall D, Kelleher M, Sanchez O, Mathews B, et al. Hospitalist-Operated Compression Ultrasonography: a Point-of-Care Ultrasound Study (HOCUS-POCUS). J Gen Intern Med. 2019;34(10):2062-7.
Pedraza Garcia J, et al. Comparison of the Accuracy of Emergency Department-Performed Point-of-Care-Ultrasound (POCUS) in the Diagnosis of Lower-Extremity Deep Vein Thrombosis. J Emerg Med. 2018.
Jang, T. B., Polites, G., Docherty, M., & Aubin, C. (2003). Resident Performed Compression Ultrasound for the Evaluation of Proximal Lower Extremity Deep Vein Thrombosis: Fast, Accurate, and Timely. Academic Emergency Medicine, 10(5), 427.