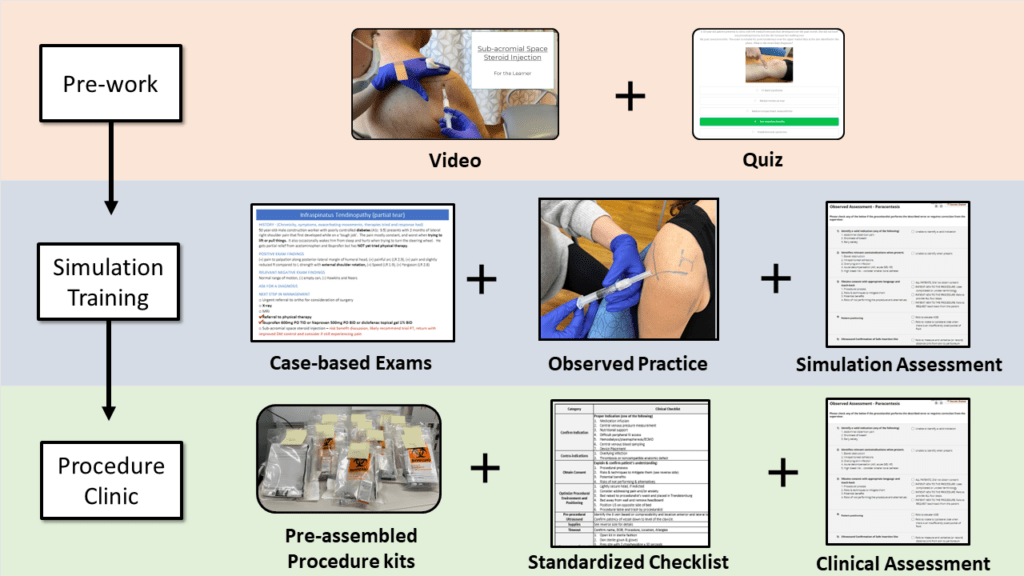
Learners watch a video and complete a digitally accessible quiz to assess their baseline knowledge and prime their learning before the simulation.


The exact structure of an individual simulation will depend upon the procedure being taught. Regardless of procedure, it is critical that both the learner and instructor treat the simulation like a true clinical encounter. This provides more opportunity for the instructor to identify and correct learner errors, and to reduce the extraneous cognitive load for the learner when they perform the procedure in a clinical setting.
Basic structure that can be applied to any procedure simulation:
1. Discuss the cognitive steps required to prepare for the procedure (indications and contraindications, risks and benefits, patient and provider positioning) as a group.
Optional: Perform case-based practice of relevant physical exam skills (e.g. MSK exams) with clinical decision making.
2. Identify anatomical landmarks (with ultrasound for relevant procedures) and practice marking the insertion site.
3. Prepare supplies.
4. Practice technical steps (instructor may first model proper technique).
5. Learner repeats above steps until they have demonstrated the targeted competence based on a predetermined minimum passing score (mastery learning).

Photo above: Learner identifies landmarks and marks an injection site

Photo above: Learner simulates injection using a capped needle