Published April 2022
Jennifer Doran, MD1, Brandon Fainstad, MD2
Section editor: Carolina Ortiz-Lopez, MD3
1 Resident, Internal Medicine, University of Colorado, 2 Assistant Professor, General Internal Medicine, University of Colorado, 3 Assistant Professor, Hospital Medicine, Co-Director for Internal Medicine Resident POCUS Training, University of Colorado
Objective(s)
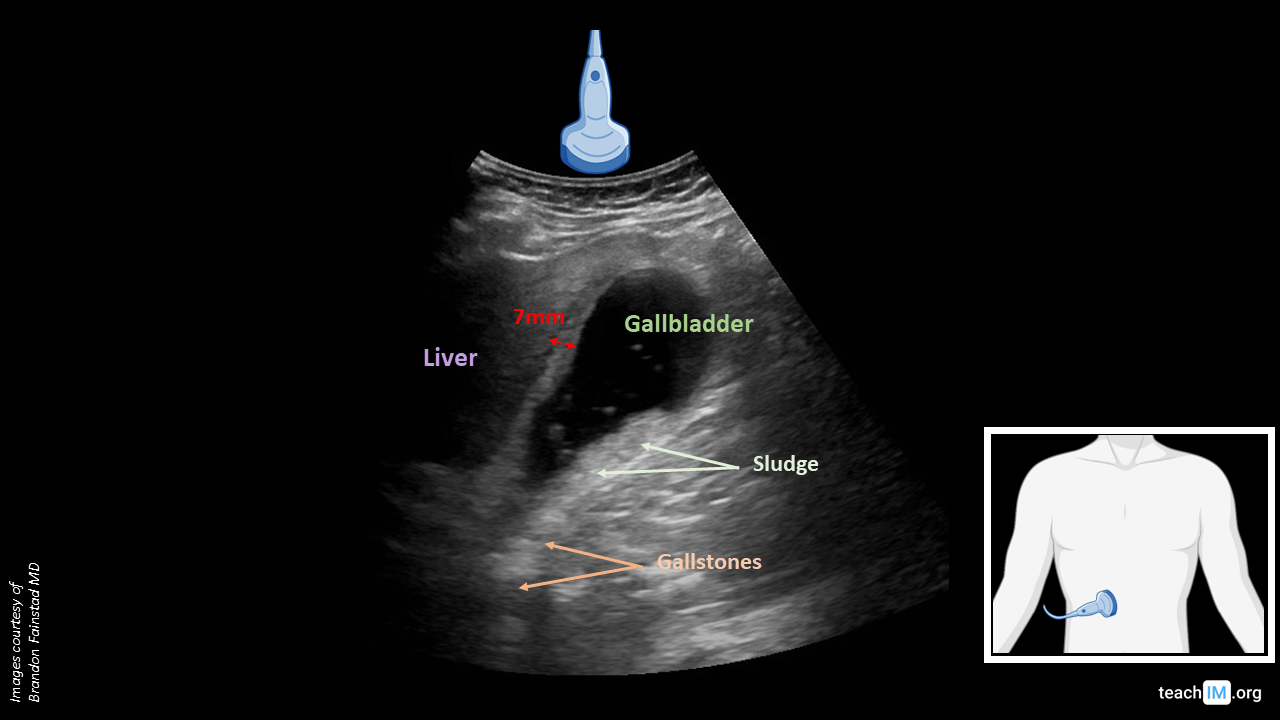
- To identify key structures including liver, gallbladder, and biliary stones.
- To recognize which probe should be used for biliary pathology
Teaching Instructions
Plan to spend 5-10 minutes familiarizing yourself with the animations of the PowerPoint and the key findings of this POCUS clip.
Instructions: Download the PowerPoint presentation file (videos do not work in the browser viewer) and have the image pulled up in presenter mode before learners look at the screen, to avoid revealing the diagnosis. Ask learners to discuss with their neighbors the answer to each question for about 30 seconds. Then advance through the animations and teaching points to the next question, and repeat. You can go back to prior graphics and questions by using the back arrow on the keyboard or by scrolling back on the mouse wheel. This should take no more than 5-10 mintues.
Image interpretation: Likely obstructing gallstones at neck of gallbladder with layering and floating sludge material. The gallbladder wall is thickened at 7mm without pericholecystic fluid, consistent with cholecystitis in the correct clinical context.
Clinical diagnosis: Cholelithiasis with acute cholecystitis
Teaching:
- Acute epigastric and right upper quadrant pain has a limited differential including gallstone disease, which can be easily evaluated at bedside with point-of-care ultrasound.
- A non-fasting gallbladder is difficult to visualize due to contractoin and increased instestinal gas.
- Gallstones are identified as gravity dependent echogenic material with a hyperechoic rim and an echogenic shaddow. The precense of a shaddow is key to differentiating it from other echogenic material in the gallbladder such as a polyp or sludge.
- While biliary sludge is typically layering, dependent material it can have varying echogenicity and may form discrete structures called tumefactive sludge. While sludge may also cause duct obstruction, it is much less likely. The best way to differentiate these structures form stones is that tumefactive sludge will NOT have an echogenic shaddow.
- Gallstones in the neck of the gallbladder with persistent symptoms, positive murphey sign and features of systemic inflammation are all suggestive of cholecystitis.
- While visulualization and measurement of the common bile duct (CBD) is a technically difficult maneuver often requring a high resolution ultrasound machine, choledocholithiasis and cholangitis are unlikely in the absence of LFT abnormalities.
Presentation Board
Take Home Point
- A thickened gallbladder is defined as >3mm but may be due to surrounding inflammation or low oncotic pressure rather than cholecystitis.
- Gallstones have a hyperechoic rim and, most importantly, an echogenic shadow that helps differentiate it from tumefactive sludge and polyps.
References
- Soni NJ. Point of care ultrasound. 2nd edition. ed. St. Louis, MO: Elsevier; 2019
- Case image courtesy of Dr Chris O'Donnell, Radiopaedia.org, rID: 19516