Published April 2022
1 Resident, Internal Medicine, University of Colorado, 2 Assistant Professor, General Internal Medicine, University of Colorado
Objective(s)
- Identify systolic dysfunction in the PLAX view and use end-point septal separation (EPSS) to characterize the severity.
- List the common valvular conditions and measuring errors that lead to overestimation of an EPSS.
Teaching Instructions
Plan to spend 5-10 minutes familiarizing yourself with the animations of the PowerPoint and the key findings of this POCUS clip.
Instructions: Download the PowerPoint presentation file (videos do not work in the browser viewer) and have the image pulled up in presenter mode before learners look at the screen, to avoid revealing the diagnosis. Ask learners to discuss with their neighbors the answer to each question for about 30 seconds. Then advance through the animations and teaching points to the next question, and repeat. You can go back to prior graphics and questions by using the back arrow on the keyboard or by scrolling back on the mouse wheel. This should take no more than 5-10 mintues.
Ultrasound interpretation: Severely reduced LVEF with enlarged left atrium.
Diagnosis: Acutely decompensated heart failure with reduced ejection fraction (HFrEF)
Teaching:
- Left atrial enlargement – The LA is much larger than the LVOT and RV (rule of thirds).
- Reduced systolic function – The cross-sectional area of the LV chamber does not decrease much in size and the walls do not thicken.
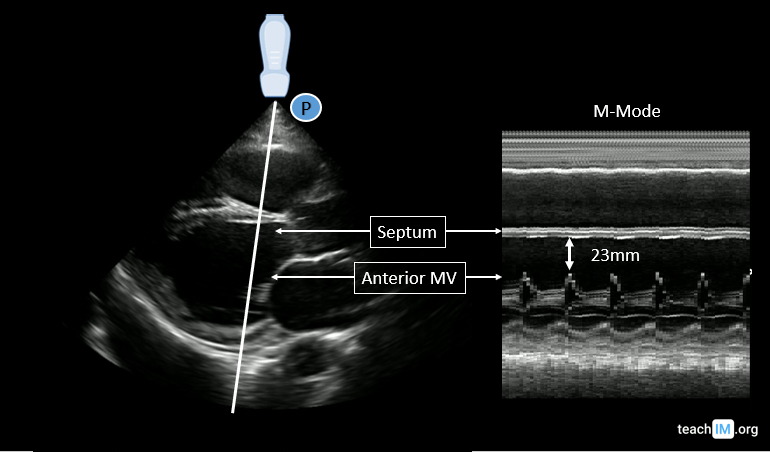
- E-point septal separation – The minimum distance between the anterior mitral valve leaflet and the interventricular septum. In patients with normal systolic function, approaches or touches the septum. An EPSS distance of <7mm is considered normal. EPSS <7mm suggests normal systolic function, with increasing distances correlating with more severe systolic dysfunction (lower EF). A EPSS > 13mm suggests mod-severely reduced EF <35%. However, the EPSS may be falsely increased in the setting of valvular disease (mitral stenosis or aortic regurgitation) or if the M-mode line is misaligned. It is important to first evaluate global cardiac function (GCF) before calculating an EPSS to avoid overinterpreting the EPSS measurement.
Presentation Board
Take Home Point
- E-point septal separation (EPSS) is measured with M-mode along the distal portion of the anterior mitral valve.
- Increasingly large EPSS measurements correlate with worse systolic function:
- An EPSS <7mm suggests a normal systolic function.
- An EPSS >13mm suggests mod-severely reduced EF
- Mitral stenosis, aortic regurgitation or a misaligned M-mode may over-estimate EPSS.
References
Soni NJ, Franco R, Velez MI, et al. Ultrasound in the diagnosis and management of pleural effusions. J Hosp Med. 2015;10(12):811-816. doi:10.1002/jhm.2434
McKaigney CJ, Krantz MJ, La Rocque CL, Hurst ND, Buchanan MS, Kendall JL. E-point septal separation: a bedside tool for emergency physician assessment of left ventricular ejection fraction. Am J Emerg Med. 2014 Jun;32(6):493-7. doi: 10.1016/j.ajem.2014.01.045. Epub 2014 Feb 3. PMID: 24630604.