Published April 2022
Section editor: Josephine Cool, MD3
1 Resident, Internal Medicine, University of Colorado, 2 Assistant Professor, General Internal Medicine, University of Colorado, 3 Instructor at Harvard Medical School, Director of Procedural and Ultrasound Education in Hospital Medicine and Director of Ultrasound Education for Internal Medicine Residency, Beth Israel Deaconess Medical Center
Objective(s)
- Identify characteristics, include the “D-sign”, of right ventricular strain in the parasternal short axis (PSAX) view.
- Generate a differential diagnosis for RV strain.
- Determine the appropriate next steps in management when a massive PE is suspected based on clinical presentation and focused cardiac assessment.
Teaching Instructions
Plan to spend 5-10 minutes familiarizing yourself with the animations of the PowerPoint and the key findings of this POCUS clip.
Instructions: Download the PowerPoint presentation file (videos do not work in the browser viewer) and have the image pulled up in presenter mode before learners look at the screen, to avoid revealing the diagnosis. Ask learners to discuss with their neighbors the answer to each question for about 30 seconds. Then advance through the animations and teaching points to the next question, and repeat. You can go back to prior graphics and questions by using the back arrow on the keyboard or by scrolling back on the mouse wheel. This should take no more than 5-10 mintues.
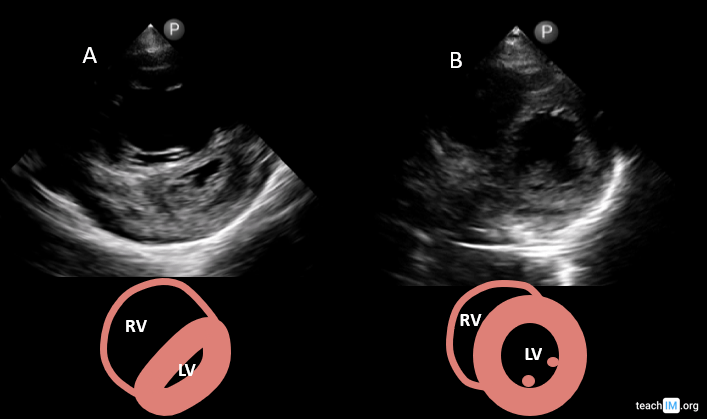
Image interpretation: Parasternal short axis (PSAX) with dilated RV with flattened intraventricular septum (“D-sign) suggestive of RV strain.
Clinical diagnosis: RV strain in the setting of acute chest symptoms and shock, concerning for a massive pulmonary embolus.
Teaching:
- The parasternal short axis (PSAX) and apical 4-chamber (A4C) are the preferred views to identify an elevated RV pressure or RV strain.
- In a normally functioning heart, the LV size, presure and wall thicknes is greater than the RV. If RV pressures become greater than the LV (due to increased RV afterload or RV systolic dysfunction) the RV size will increase and the intraventricular septum will flatten.
- In the PSAX this is best identified by the “D-sign” where the LV takes on a shape of a “D” rather than its normal circular shape.
- In the A4C an RV pressure > LV pressure is identified by their relative size (RV > LV). This will be discussed in greater detail in a sperate case.
Presentation Board
Take Home Point
- The PSAX is the preferred view to identify RV strain with a dilated RV and flattened interventricular septum or “D-sign”.
- The most common differential RV pressure > LV pressure includes:
- Acute pulmonary embolus
- Chronic pulmonary hypertension
- RV systolic dysfunction
- Pulmonic valve disease
References
Alerhand S, Sundaram T, Gottlieb M. What are the echocardiographic findings of acute right ventricular strain that suggest pulmonary embolism? Anaesth Crit Care Pain Med. 2021 Apr;40(2):100852. doi: 10.1016/j.accpm.2021.100852. Epub 2021 Mar 26. PMID: 33781986.
Ruxandra Jurcut, Sorin Giusca, André La Gerche, Simona Vasile, Carmen Ginghina, Jens-Uwe Voigt, The echocardiographic assessment of the right ventricle: what to do in 2010?, European Journal of Echocardiography, Volume 11, Issue 2, March 2010, Pages 81–96, https://doi.org/10.1093/ejechocard/jep234