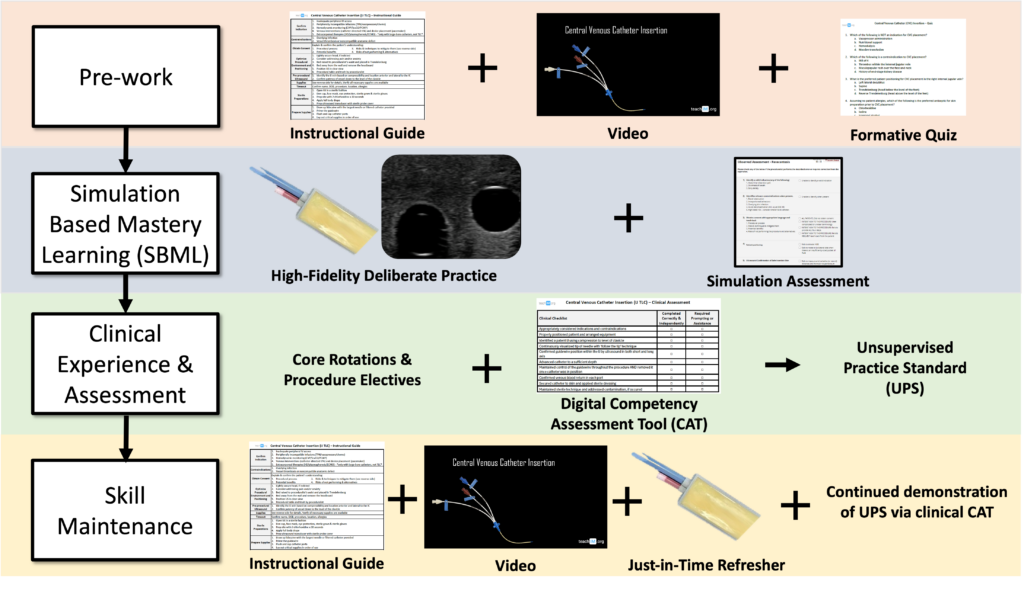
Learners watch a video and complete a digitally accessible quiz to assess their baseline knowledge and prime their learning before the simulation.


It is valuable to time the resident’s simulation training near their expected clinical practice of the procedure. This can be incorporated within the relevant rotation (E.g., CVC simulation during the first week of ICU rotation) or during protected educational sessions in a predictable block schedule that allows programmatic implimentation. Simulation training is often most limited by the availability of high-fidelity task trainers and effective instructors. We provide instructions for DIY 3D printed casing for balistics gel models that enable a mobile and cost-concious solution.
It is critical that both the learner and instructor treat the simulation like a true clinical encounter. This provides more opportunity for the instructor to identify and correct learner errors, and to reduce the extraneous cognitive load for the learner when they perform the procedure in a clinical setting.
Basic simulation structure:
1. Discuss the cognitive steps required to prepare for the procedure (indications and contraindications, risks and benefits, patient and provider positioning) as a group.
2. Identify anatomical landmarks (with ultrasound for relevant procedures) and practice marking the insertion site.
3. Prepare supplies.
4. Instructor demonstrates proper technique
5. Learner practices technical steps with iterative feedback
Optional: practice troubleshooting scenarios and/or relevant case-based physical exams (e.g., for MSK procedures)
6. Learner repeats above steps until they have demonstrated the targeted competence based on a predetermined minimum passing score (mastery learning).

Photo above: Learner identifies landmarks and marks an injection site

Photo above: Learner simulates injection using a capped needle
Residents are exposed to clinical procedures during their core internal medicine rotations, where they perform procedures as they arise in the course of routine patient care. While this opportunistic model is the traditional norm, it rarely ensures that residents gain sufficient experience across all procedures of interest to reach competency for independent practice.
To address this gap and support residents in meeting their personal procedural competency goals, we recommend offering dedicated, procedurally focused electives. These may include structured experiences such as a procedure clinic, women’s health elective, rotations with a hospital-based medical procedure service, or time in the catheterization lab. Ideally, each of these settings would incorporate direct observation and real-time competency assessments. These assessments should be digitally documented and shared with the residency program to provide clear insight into each trainee’s progress and to inform decisions about their readiness for independent practice.
CVC example:
Skill degradation in procedures can begin as early as three months post-training, particularly for complex or infrequently performed interventions (Huang et al., 2024). Prior experience offers some protection, but even expert clinicians benefit from periodic refreshers (Kahol et al., 2011). Our approach combines on-demand digital resources, just-in-time task trainer access, and SBML-based annual sessions to help mitigate procedural skill decay (McGaghie et al., 2011; Andreatta et al., 2011). Furthermore, because many trainees encounter limited procedural volume, annual clinical assessments remain crucial to ensure readiness for independent practice (Barsuk et al., 2009).